
Phases of Healing Improvements in Timing and Quality of Healing Problems and Residual Characteristics
There are many published journal articles and books pertaining to the topic of “Soft Tissue Injury and Repair.” My favorites include:
- Studies on development of connective tissue in transparent chambers in rabbit’s ear; American Journal of Anatomy; 1940.
- Orthopaedic Medicine, Diagnosis of Soft Tissue Lesions; 1982.
- Acute soft tissue injuries; Australian Family Physician, 1982.
- Sports Medicine: Prevention, Evaluation, Management, and Rehabilitation; 1983.
- Normal ligament Properties and Ligament Healing; Clinical Orthopedics and Related Research; 1985.
- Acute soft tissue injuries-a review of the literature; Medicine and Science of Sports and Exercise; 1986
- Injury and Repair of the Musculoskeletal Soft Tissues; American Academy of Orthopaedic Surgeons;
- Wound Healing, Biochemical & Clinical Aspects; 1992.
- Continuous Passive Motion, A Biological Concept for the Healing and Regeneration of Articular Cartilage, Ligaments, and Tendons; From Origination to Research to Clinical Applications; 1993.
- Effects of Early Motion on Healing of Musculoskeletal Tissues, Hand Clinics; 1996.
- Scar Formation and Ligament Healing; Canadian Journal of Surgery; 1998
- Immobilization or Early Mobilization After an Acute Soft-Tissue Injury?; The Physician And Sports Medicine; 2000.
- Cells, Tissues, and Disease: Principles of General Pathology, 2004.
- The Basics of Soft Tissue Healing and General Factors that Influence Such Healing; Sports Medicine Arthroscopic Review; 2005.
- Orthopedic Biology and Medicine; Repair and Regeneration of Ligaments, Tendons, and Joint Capsule; Humana Press, 2006.
- Fascia: The Tensional Network of the Human Body; The Scientific and Clinical Applications in Manual and Movement Therapy; 2012.
Phases of Healing
The article I have seen referenced (and personally used in numerous contexts) most often was published in 1986 in the journal Medicine and Science in Sports and Exercise by Australian physician John Kellett, MD, and titled (6):
Acute soft tissue injuries--a review of the literature
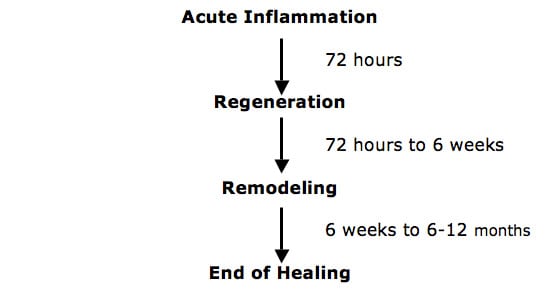
In this article, Dr. Kellett describes the pathological processes of soft tissue healing as following three distinct phases:
- Phase 1: the acute inflammatory phase
- Phase 2: the repair phase
- Phase 3: remodeling phase
The phases of soft tissue injury repair are:
Phase 1: The Acute Inflammatory or Reaction Phase
This phase of healing lasts up to about 72 hours. It is characterized by vasodilation, immune system activation of phagocytosis to remove debris, the release of prostaglandins and inflammation.
The prostaglandins play a prominent part in pain production and increased capillary permeability (swelling).
The wound is hypoxic because the blood vessels have been disrupted, but immune system macrophages perform their phagocytosis duties anaerobically.
Phase 2: The Repair or Regeneration Phase
This phase begins at about 48 hours and continues for about 6 weeks. This phase is characterized by the synthesis and deposition of collagen, which literally glue the margins of the healing breach together.
The collagen that is deposited in this phase is not fully oriented in the direction of tensile strength. Rather, is laid down in an irregular, non-physiological pattern. Dr. Kellett states:
This phase is “largely one of increasing the quantity of the collagen” but this collagen is not laid down in the direction of stress.
Phase 3: The Remodeling Phase
This phase may last up to “12 months or more.” Dr. Kellett stresses that the remodeling phase of healing is critical for establishing the ultimate quality and functional capabilities of the healed tissues. He states:
“The collagen is remodeled to increase the functional capabilities of the tendon or ligament to withstand the stresses imposed upon it.”
This phase is largely “an improvement of the quality” (orientation and tensile strength) of the collagen.
Stages of Healing Following Soft Tissue Injury
In support of the healing steps detailed by Dr. John Kellett, Physician Kevin Hildebrand, MD, and colleagues, from the University of Calgary, Alberta, Canada published a study in the journal Sports Medicine Arthroscopic Review, in 2005 titled (14):
The Basics of Soft Tissue Healing and
General Factors that Influence Such Healing
Dr. Hildebrand and colleagues point out that wound healing following overt injury to a tissue follows general ‘‘rules’’ irrespective of the tissue involved. These “rules” are similar but somewhat more detailed than those outlined by Dr. Kellett. They include:
Phase 1: The Inflammatory
Following acute injury there is bleeding into the area of injury and pain. “Hemostasis is restored by the formation of a fibrin clot, which prevents further bleeding and serves as a provisional matrix for migrating cells.” This clotting cascade results in the release of inflammatory molecules and inflammatory cytokines from cells such as platelets. There is an influx of fibroblasts, which sets the stage for the second phase of the repair process.
Phase 2: The Matrix Deposition Phase
The fibroblasts produce collagen proteins that bridge the damaged area with the residual endogenous ligament tissue. “The tissue deposited early after injury appears to be an attempt to bridge the damaged area without regard to what was present before injury.”
Phase 3: The Remodeling Phase
“The remodeling phase is a slow process and is accompanied by alterations not only in matrix remodeling, but also gene expression, cellularity, vascularity, and innervation.” The scar tissue in a ligament “undergoes a protracted process where the initially deposited material seems to be turning over and the organization of collagen fibrils become more oriented along the long axis of the ligament.” “Because the remodeling phase occurs slowly, and may take months (i.e., skin) or years (i.e., tendon and ligament).” [Important]
Last year (2012), Robert Schleip, PhD, (Division of Neurophysiology, Ulm University, Germany) and colleagues, published an excellent and very detailed book on soft tissues, titled (16):
Fascia
The Tensional Network of the Human Body
The Scientific and Clinical Applications in Manual and Movement Therapy
In this book, they add to the details of the principles of soft tissue injury and repair. Specifically, they state: “Wound healing is divided into three or four phases:”
Phase 1A: The Vascular Inflammatory Phase
This phase begins immediately after injury and last 0 – 2 days. It is characterized by bleeding into the tissue.
Phase 1B: The Cellular Inflammatory Phase
Fibroblasts migrate into the injury area. This phase lasts 2 – 5 days.
Phase 2: The Proliferation Phase
This phase begins at the fifth day and lasts about 21 – 28 days. “The proliferation phase in poorly perfused tissue such as tendon, ligament, meniscus, or intervertebral disc can last up to 6 weeks.”
In this phase, wound closure occurs with a network of collagen fibers. “For this collagen network to attain an almost identical construction of the original tissue, the tissue in this phase of would healing must be confronted with its normal physiological stress.”
Phase 3: The Consolidation Reconstruction Phase
This phase begins between days 21 – 28, and continues to about day sixty.
Phase 4: The Remodeling / Maturation Reconstruction Phase
This phase begins at about day 60 and continues for about a year. “Stress on the tissue should now be slowly increased to push ahead the reconstruction of unstable type III collagen to stable type I collagen and return the tissue to its original stability.”
Improvements in Timing and Quality of Healing
There are a number of variables that influence the timing and quality of healing.
Dr. Kellett notes (6):
“Cryotherapy (crushed ice) for 10 to 20 min, 2 to 4 times/day for the first 2 to 3 days is helpful in promoting early return to full activity.” “Numerous studies have shown the effectiveness of ice therapy in reducing the pain and period of disability to soft tissue injuries.” In contrast, “early heat treatment leads to an increase in the blood flow to the injured area with an exaggerated acute inflammatory response.”
“The advantages of cryotherapy in treating soft tissue injuries have been well documented.” Ice within 48 hours of injury reduces disability of ankle sprains from 15 days to 10 days.
“Early mobilization, guided by the pain response, promotes a more rapid return to full activity.”
“Early mobilization, guided by the pain response, promotes a more rapid return to full functional recovery.”
“Progressive resistance exercises (isotonic, isokinetic, and isometric) are essential to restore full muscle and joint function.”
Following this acute inflammatory phase and largely guided by the pain response of the patient, early mobilization is commenced, based upon the premise that the stress of movement on repairing collagen is largely responsible for the orientation and tensile strength of the tendons and ligaments.
The goal of stressing repairing tissues with controlled motion is to induce adaptive response of functionally stronger connective tissues. However, excessive stressing of the repairing tissues may result in further damage. Consequently, any sign or symptom which suggests a worsening of the injury (severe pain) is a clear indication to reduce the motion stress on the tissues.
The strength of repaired ligaments is proportional to the mobility of the ligament, resulting in larger diameter collagen fiber bundles and more total collagen. “Collagen fiber growth and realignment can be stimulated by early tensile loading of muscle, tendon, and ligament.”
•••••••••
In 1998, Drs. Hildebrand and Frank note (11):
“Motion in stable joints improves the biomechanical properties of healing ligaments compared with immobilization of joints.” “The mechanism presumably involves the application of controlled forces; too little or too much force is detrimental.”
•••••••••
In 2005, Dr. Hildebrand and colleagues note (14):
“The large scar tissue mass gradually remodels, likely under the influence of the mechanical environment.”
“Maturation of the scar tissue requires mechanical loading to continue the remodeling phase of healing.”
“Normal connective tissues that function in a mechanically active environment (actually most tissues) subscribe to the ‘‘use it or lose it’’ paradigm of tissue integrity.” “Increased loading leads to adaptation, whereas decreased loading below a threshold leads to atrophy.” “The same principle likely also holds for scar tissue and immobilization beyond the initial phases of healing could have a detrimental impact on outcome.”
“Mechanobiology is likely important in the healing outcome in tissues such as ligaments, tendons, and related tissues. That is, depriving healing ligaments of mechanical loading likely has a detrimental impact on healing outcome.”
•••••••••
Dr. Schleip and colleagues note (16):
“For this collagen network to attain an almost identical construction of the original tissue, the tissue in this phase of would healing must be confronted with its normal physiological stress.”
“Stress on the tissue should now be slowly increased to push ahead the reconstruction of unstable type III collagen to stable type I collagen and return the tissue to its original stability.”
“Because connective tissue consists predominantly of proteins, the take-up of protein through nutrition is very important.”
“Matrix and cells are found in a continuous dialogue and are dependent on each other.” “The forces on the network of collagen and elastic fibers and ground substance are transferred to the cell membranes via link proteins. The cell is informed by these signals and is stimulated to keep synthesizing new matrix components. This rebalances the physiological breakdown of the matrix and the tissue retains its stability and mobility. A reduction in the load stimulus leads as a result to reduced synthesis activity of the cells and thus to a loss of matrix components.”
“This produces a lower level of stability and limited mobility because of the formation of pathological cross links. An important task for the therapist is to apply gradually increasing levels of force without causing pain, in order to promote the healing and regeneration processes and in this way restore mobility and stability.”
•••••••••
Problems and Residual Characteristics
Most healed soft tissue injuries are asymptomatic. However, it is universally accepted that the healed tissue is weaker than the pre-injured tissue. Consequently, acute flare-ups of pain or exacerbations of pain and/or spasm often occur as a consequence of increased use or stress of the once injured but now healed tissues. Good early treatment improves the quality and timing of soft tissue injury. Best early treatment appears to include ice and early controlled motion that does not move the tissues into pain.
The chronic tissue residuals following trauma and healing are histologically provable. Common terminology to describe them includes “scar, fibrosis, fibrosis of repair, adhesions,” etc. A collection of these principles follows:
Dr. Kellett notes (6):
“The micropathology of acute soft tissue trauma has been investigated. Healing of ligaments and soft tissue injuries in general has been shown to occur by fibrous repair (scar tissue) and not by regeneration of the damaged tissue.”
“Normal ligaments are composed of type I collagen, whereas damaged (and healed) ligaments contain a large proportion of immature type III collagen which is deficient in the number of cross-linkages between and within the tropocollagen subunits.”
The remodeled scar is deficient in both content and quality 40 weeks after injury, as there is a plateau in scar collagen concentration at about 70% of normal.
•••••••••
In 1998, Drs. Hildebrand ad Frank note (11):
“Injuries to ligaments induce a healing response that is characterized by the formation of a scar.” This “scar tissue is weaker.”
“Ligament healing is characterized by the formation and remodeling of scar tissue that is weaker than normal ligament owing to alterations in biochemical composition and structural organization.” “The scars have a greater amount of inferior strength tissue compared with that of normal” ligaments.
“The structural strength and stiffness, stress and tissue quality continue to improve up to 12 months after injury, but after that time only relatively small increases are made. However, the material properties of the ligament scar do not return to normal even after 2 years.”
Residual scar tissue behaves with “abnormal biomechanical, biochemical and ultrastructural properties.”
“The return of joint function after injury does not mean that the ligament has healed.”
“Ligament healing in what may be considered to be the best case scenario is characterized by a scar material with inferior tissue quality, with changes in biochemical and histologic properties, that does not regenerate a normal ligament even after 2 years of healing.”
The ligament scar affects the associated joint function.
•••••••••
In 2005, Dr. Hildebrand and colleagues note (14):
“Whereas wound healing generally leads to a repair of the injured site, it does not lead to tissue regeneration. This difference between repair and regeneration has influence on tissues such as ligaments and tendons that function in a mechanically active environment.”
The repair process can lead to a loss of function, primarily from scar tissue, and this can occur in both musculoskeletal and visceral tissue (heart, lung, kidney, liver).
“The remodeling phase is a slow process and is accompanied by alterations not only in matrix remodeling, but also gene expression, cellularity, vascularity, and innervation.” “Because the remodeling phase occurs slowly, and may take months (i.e., skin) or years (i.e., tendon and ligament).”
“Even after protracted time post-injury, the mechanical properties of a scar tissue in a ligament … is still compromised compared with normal.”
“The scar tissue may be functional for most activities even though it is not ‘normal’.” [Fails during high demand activities]
The scar cells in the healing ligament are different from normal cells and therefore the scar is intrinsically different.
‘‘Scar-like’’ tissue is “functionally ineffective.”
“Some tendon and ligament injuries lead to formation of scar tissue that is partially functional, but to regain as much function as possible requires physiotherapy to ‘facilitate’ the return to function after the scar tissue has formed.”
The inflammatory response associated with overt injury or surgery can lead to formation of adhesions, where “the ligament/tendon scar tissue is ‘‘bonded’’ to the surrounding tissue and thus, such restrictions compromise function in situations where movement is required.”
“The size of the wound and the resulting scar tissue has a dramatic impact on the biomechanical outcome.”
“It is readily apparent that wound healing in the adult under the most optimal conditions should be considered tissue repair not regeneration.” “For tissues like a ligament or tendon, the mechanical outcome may be less than ideal, depending on the expectations of tissue use post-injury and the occurrence of side-effects such as adhesions.”
Additionally, Dr. Hildebrand and colleagues discuss factors that impair soft tissue healing. These factors cause some patients to heal slowly or incompletely with more functional residuals. These factors include:
- Older age
- Female Sex
- Genetics
- Tissue history (prior injuries, scar tissue, and disease states)
- Diabetes
- Disc injuries heal poorly, primarily as a consequence of poor blood supply
- Pregnancy
- Low Vitamin C levels
- Menstrual cycle hormonal changes
- Any reason that deprives the healing tissues from mechanical loading
- Re-injury of a prior injury or prior tissue that has sustained repetitive stress
- Excess carbohydrates that increase glycation (AGEs)
- Any treatment with corticosteroids
- Anything that exaggerates or prolongs the inflammatory response
•••••••••
Dr. William Walsh and colleagues note (15):
“Musculoskeletal soft tissues tend to heal through formation of relatively weak, disorganized scar tissue. Severe ligament sprains can be particularly problematic; even in the best case, there is a fibrotic repair response that remodels over several years, causing scar tissue that is structurally and biomechanically inferior to the normal tissue. For most soft tissues, the fibrotic repair process is thought to interfere with the possibility of regeneration.” “Soft tissues typically heal by fibrosis, potentially impairing regeneration.”
“Ligaments take longer to heal than other connective soft tissues, and the repaired ligament tissue is scarlike and inferior to normal ligament tissue both biologically and biomechanically. Furthermore, some ligament-deficient joints subsequently become unstable and can lead to lifelong disability with osteoarthritis.”
“Ligament wounds, even over 2 yr after injury, contain mainly a homogenous population of small-collagen fibrils as commonly observed in scar tissue, with a few patches of normal larger fibrils being observed. These ligaments never obtain their original biomechanical properties.”
These concepts on ligament repair have important applications for chiropractors that treat spinal trauma patients:
Soft tissue healing occurs over a period of 12 months or more. Controlled motion, including the chiropractic adjustment, is the best approach to enhance the quality of ligament healing, especially in the remodeling phase.
Ligaments and tendons heal with scar tissue (repair) as a rule, and not with normal pre-injury tissue (regeneration). This scar tissue causes permanent loss of function. Even healed ligament injuries have residual weakness.
Scar tissue is mechanically functionally inferior to normal tissue. Its inherent weakness makes the tissue prone to failure at previously normal load levels, and subsequent new trauma to scarred tissue will result in greater injury.
Scar tissue (fibrosis) is linked to the intensity of the initial inflammatory response. Consequently, early inflammation control (ice) could improve the timing and quality of healing. Scar tissue, to varying degrees, is remodelable with the application of controlled motion, which I believe includes and even requires chiropractic adjustments.
Lack of symptoms is not synonymous with full healing and functional recovery. A flare-up or exacerbation of pain after the healing process most likely will require another few quick visits to the chiropractor.
•••••••••
SUMMARY:
This review reminds us that it is well established that:
- Whiplash injury chronic pain is primarily generated by injury to the facet joint capsular ligaments.
- Facet joint capsular chronic pain can cause an abnormal psychological profile.
- The abnormal psychological profile caused by chronic facet pain can only be successfully treated if the chronic pain is successfully treated.
- Many studies conclude that litigation (hiring a lawyer) subsequent to an injury is “harmful to recovery.” However, these studies do not evaluate the concept of Reverse Causality, and hence are flawed.
- When Reverse Causality is carefully evaluated, litigation not only does not harm recovery, data suggests it actually improves recovery.
REFERENCES
- Stearns, ML, Studies on development of connective tissue in transparent chambers in rabbit’s ear; American Journal of Anatomy, vol. 67, 1940, p. 55.
- Cyriax, James, M.D., Orthopaedic Medicine, Diagnosis of Soft Tissue Lesions, Bailliere Tindall, Vol. 1, 1982.
- Oakes BW. Acute soft tissue injuries. Australian Family Physician. 1982; 10 (7): 3-16.
- Roy, Steven, M.D., and Irvin, Richard, Sports Medicine: Prevention, Evaluation, Management, and Rehabilitation, Prentice-Hall, Inc. (1983).
- Frank C, Amiel D, Woo S, Akeson W; Normal ligament Properties and Ligament Healing; Clinical Orthopedics and Related Research; June, 1985.
- Kellett J; Acute soft tissue injuries-a review of the literature; Medicine and Science of Sports and Exercise, American College of Sports Medicine, Vol. 18 No.5, (1986), pp. 489-500.
- Woo, Savio L.-Y.,(ed.), Injury and Repair of the Musculoskeletal Soft Tissues, American Academy of Orthopaedic Surgeons,(1988), p.18-21; 106-117; 151-7;
- Cohen, I. Kelman; Diegelmann, Robert F; Lindbald, William J; Wound Healing, Biochemical & Clinical Aspects, WB Saunders, 1992.
- Salter R, Continuous Passive Motion, A Biological Concept for the Healing and Regeneration of Articular Cartilage, Ligaments, and Tendons; From Origination to Research to Clinical Applications, Williams and Wilkins, 1993.
- Buckwalter J, Effects of Early Motion on Healing of Musculoskeletal Tissues, Hand Clinics, Volume 12, Number 1, February 1996.
- Hildebrand K, Frank C; Scar Formation and Ligament Healing; Canadian Journal of Surgery; December 1998; Vol. 41; No. 6; pp. 425-429.
- Kannus P, Immobilization or Early Mobilization After an Acute Soft-Tissue Injury?; The Physician And Sports Medicine; March, 2000; Vol. 26 No 3, pp. 55-63.
- Majno, Guido and Joris, Isabelle, Cells, Tissues, and Disease: Principles of General Pathology, Oxford University Press, 2004.
- Hildebrand KA, Gallant-Behm CL, Kydd AS, Hart DA; The Basics of Soft Tissue Healing and General Factors that Influence Such Healing; Sports Medicine Arthroscopic Review September 2005; Vol. 13; No. 3; pp. 136–144.
- Walsh W; Orthopedic Biology and Medicine; Repair and Regeneration of Ligaments, Tendons, and Joint Capsule; Orthopedic Research Laboratory, University of New South Wales, Sydney, Australia, Humana Press, 2006.
- Schleip R; Fascia; The Tensional Network of the Human Body; The Scientific and Clinical Applications in Manual and Movement Therapy; Churchill Livingstone, 2012.
